-
What is cognitive rehabilitation?
Cognitive rehabilitation addresses issues with cognitive functioning, and aims to strengthen these processes through a series of tasks, to be exercised on a daily basis. Cognitive functioning is defined as ‘the mental action or process of acquiring knowledge and understanding through thought, experience, and the senses’, and can include any of the following:
- Learning
- Memory
- Thinking
- Reasoning
- Memory
- Problem solving
- Decision making
- Attention
- Language
Many factors can influence cognitive functioning, including age, drinking and smoking, body mass index, depression, brain injury, and other genetic or environmental factors. We all have the same cognitive processes, but the way in which we engage in these can differ enormously from person to person.
-
Who is it helpful for?
-
How does it work?
-
What Does The Treatment Look Like?
-
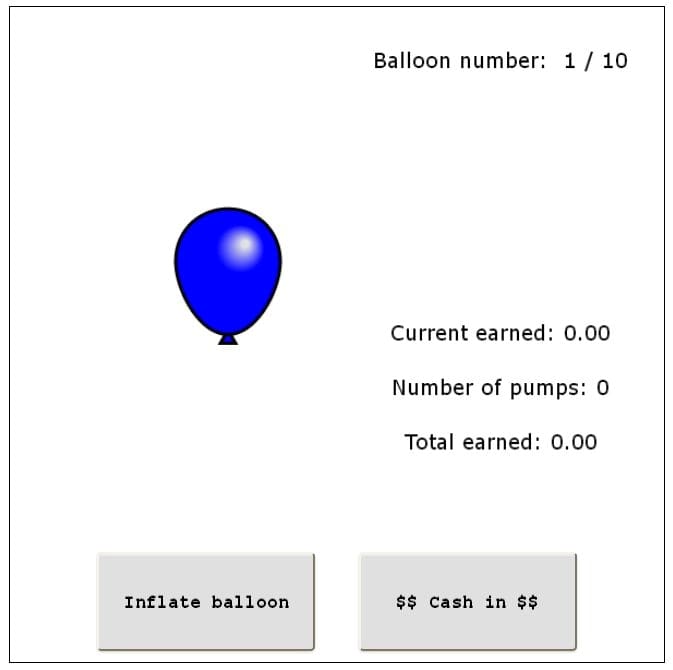
What type of exercises can I expect to do?
-
What Are The Costs?
-
References
THERAPISTS WHO TREAT COGNITIVE REHABILITATION AT PRIVATE THERAPY CLINIC

Letizia De Mori
PsychologistIQ, neurodiversity and more
Fee From: £170
Reviews (11)